How would you describe your child’s condition?
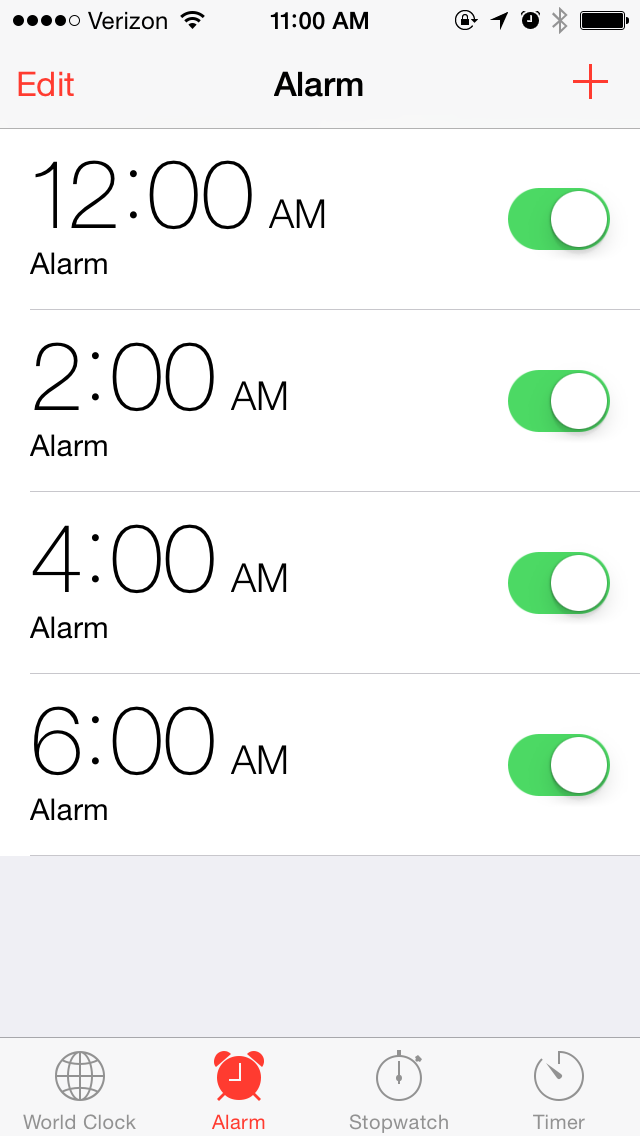
Matt: Henry has type 1 diabetes. This means that his entire life is centered around the fact that his body does not produce the insulin he needs to process glucose, so we check his blood sugar about ten times a day by poking a small needle into his finger and adding that drop of blood onto a meter that tells us what his BG (blood glucose) is. Depending on what the number is, we give him insulin, sugar, or wait. This means that we deal with low blood sugars, which are potentially, immediately, fatal; high blood sugars, which can have drastic, long-term consequences for his life; or “normal” blood sugars, which help keep him healthy. We get up every two hours every night to help maintain his blood glucose. Two weeks ago, Henry looked at me and said, “Diabetes is a hard life.” I agree.
Rachel: Our son, Henry, has an autoimmune disease, type 1 diabetes. Something triggered his beta cells to stop producing insulin, so he must take subcutaneous insulin for the rest of his life, test his blood glucose 8-12 times a day and always account for the carbs he eats with insulin. There’s never a break from type 1 diabetes, because the person with diabetes or the person’s caregiver/s is trying to replicate a job the pancreas once did.
What care for your child is required, and how do you and your partner divide this care?
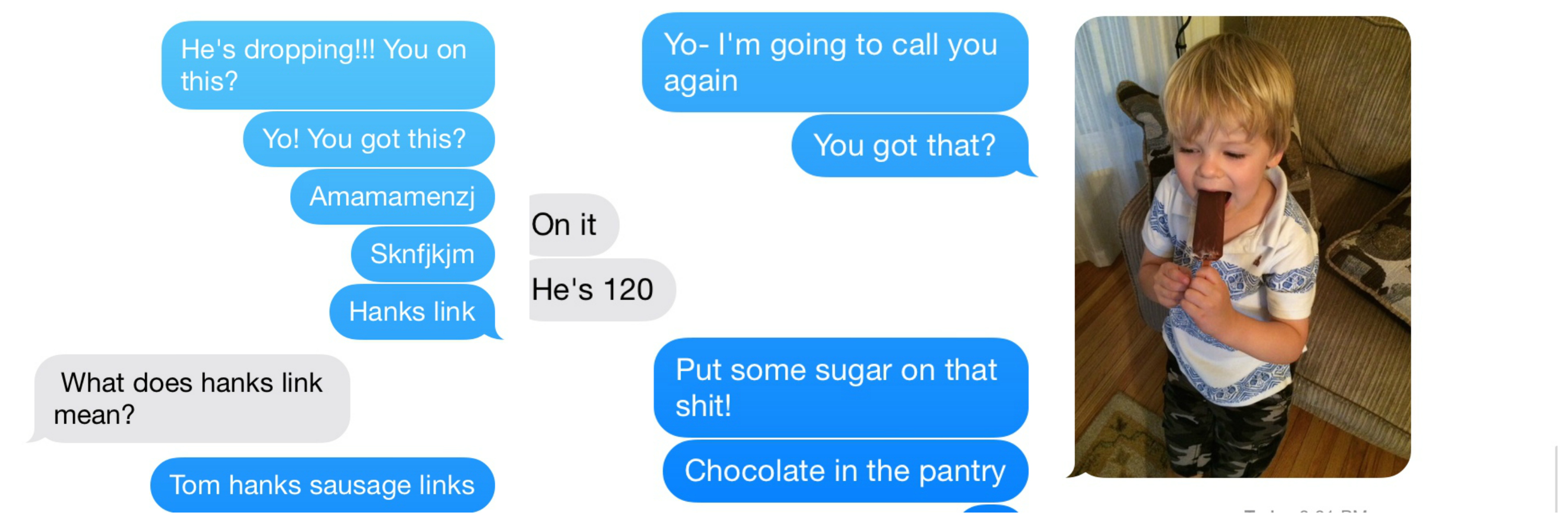
Matt: We make sure that he gets enough insulin to cover the carbs (sugars) he eats so that his blood glucose does not get too high and cause damage to his organ systems. We also make sure that his BG does not drop to a low level that could result in seizure or death. We count all of the carbs he eats and program his (miraculous) insulin pump to keep him in balance. We also change his pump site every two to three days, as well as his constant glucose monitor (CGM), another amazing device that keeps us updated on an estimate of his BG. Rachel definitively manages the difficult logistics of this care. She deals with insurance companies, refills at the pharmacy, and talking to the reps at Animas (insulin pump) and Dexcom (CGM).
Rachel and I both deal with the daily stresses of handling diabetes. We both count carbs, take BG readings, get up in the middle of the night and evenly split the duties of changing Henry’s pump and CGM sites. Henry has developed a pretty nasty allergy to the tape that holds both of these machines onto his skin, so we have to take a lot of precautions to make sure that his exposure to them is minimized. Rachel reached out to the diabetes online community and found people who helped us come up with solutions when our docs had basically given up and asked us to go to multiple daily injections.
The best balance that we have, in terms of day-to-day care, is that Rachel is very good at keeping track of what Henry needs medically and practically; she amazes me with how much she has learned about diabetes and its care— and I am helpful in the ways that I try to create some distance from a life with diabetes and a “normal” life for Henry. I’m probably more likely to encourage us to get ice cream or wait to change a site— this balance only functions because of how hard Rachel works.
Rachel: In the wise words of Kenny Rogers, “Know when to hold ‘em, / Know when to fold ‘em / Know when to walk away / Know when to run.” I know when to hold ‘em, which comes in handy with the rigor and attention counting carbs and dosing insulin requires. Matt knows when to fold ‘em and let Henry live the life of a five year old with birthday parties, extra ice cream, and a day longer with a site. Henry will need both of these skills as he learns to live and manage his diabetes. Balancing diabetes is an art and a science, so I’m the science while Matt’s the art. Matt and I both know when to walk or run away from a negative comment, failing site, or excessive carb scene.

Team Pancreas
How has being a caregiver changed your relationship?
Matt: I don’t think it’s changed us fundamentally. We don’t always agree about everything to do with Henry, but we always talk about why we think a certain action is best in the certain moment. Ultimately, we are both focused on making sure that Henry is safe and protected. Chronic conditions are definitely an added stressor, and I’m sure that we get a little snappier at 3:00 in the morning, but we are both committed to each other and to caring for Henry.
Rachel: A lot, but a little. A lot because we are now caregivers for our son, who has a chronic condition, but not a lot because we decided to become partners and then parents together long before diabetes entered our lives, so we’ve mostly figured out how to handle stress and difficulty. A day to day difference is struggling with time, because everyday actions, such as preparing for a trip or eating at a restaurant, are now more complex and require discussion, preparation, and planning. We have to depend on each other more.
Describe a caregiver technique you and your partner do differently.
Rachel: We both do really hard things. For the past 18 months I’ve put in Henry’s pump site, which feels like I’m stabbing him with a giant needle. Henry anticipates site changes, and it’s just awful to know that I’m causing my child physical pain, even if it’s for treatment. When Henry asks something like, “Will I have diabetes when I’m a grown up?” Matt can answer this question honestly and have Henry laughing within a few minutes, whereas I have to leave the room because I don’t trust myself to answer without getting choked up.
Matt: We have split things up, but we talk or text at least two or three times a day about his care when we are both at work. Changing the site of Henry’s pump is stressful because of the precautions we have to take with his skin and because he dreads them. We put Lidocaine on his skin to decrease the pain but they still worry him. I prep the area on his skin and get the pump primed to administer insulin and hold him while Rachel actually inserts the pump.
In twenty words or less, describe your partner’s caregiving superpower.
Rachel: Matt’s superpower is levity that inspires patience and laughter, needed in the shadow of a wrong number at the right moment.
Matt: Rachel’s superpower is her love for Henry and how this gives her a laser-like focus on keeping him alive.